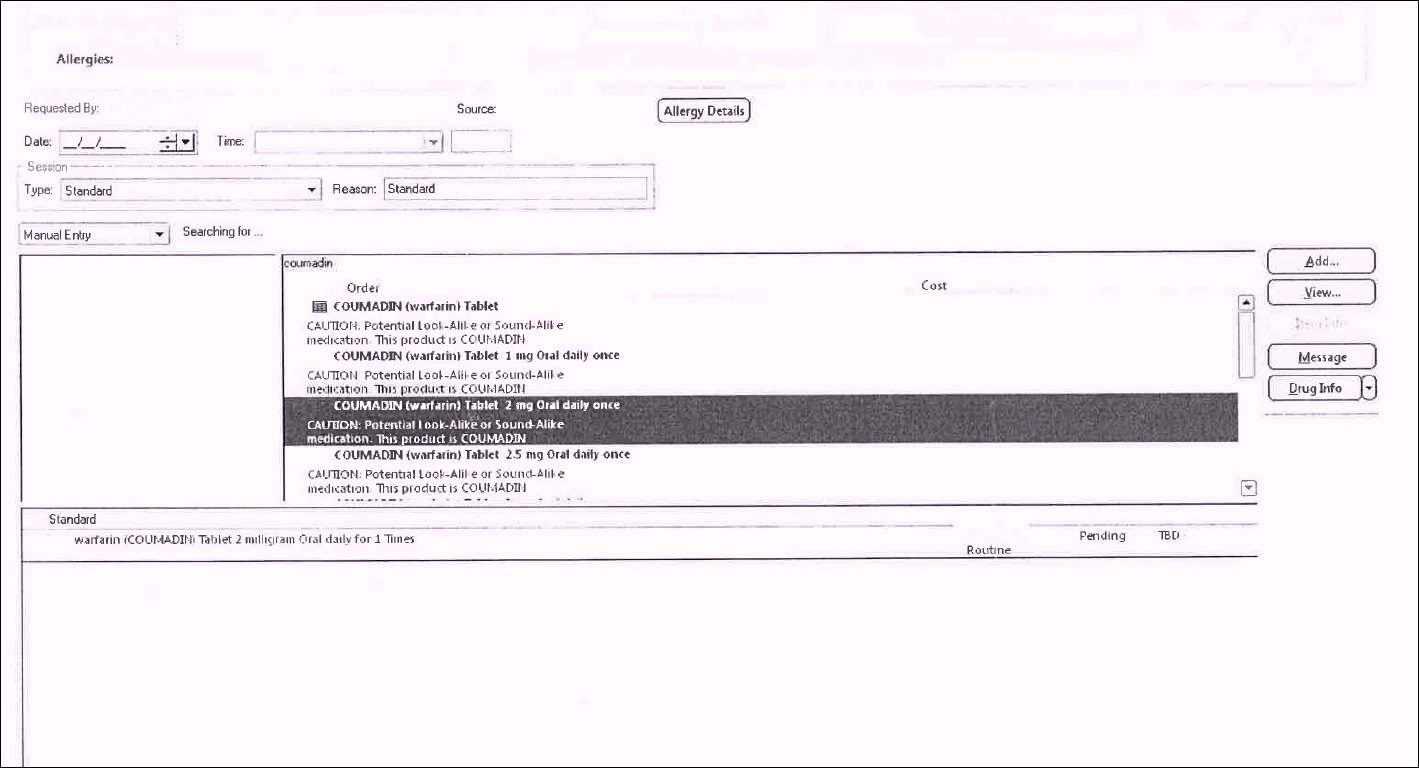
CPOE selection screen for crucial blood thinner, coumadin (Warfarin). Click to enlarge.
This order entry screen, from a production system (of a vendor whose stock price has recently taken a dive) shows the following. In all fairness, I do note it's unclear if the vendor or the customer's configuration "experts" were responsible for this:
COUMADIN (warfarin) tablet 2 mg Oral daily once.
CAUTION: Potential look-Alike or Sound-Alike medication - this product is COUMADIN
CAUTION: Potential look-Alike or Sound-Alike medication - this product is COUMADIN
with similar entries for other doses.
Below and not indented as is the selection, where the clinician is liable not to look very carefully, is the helpful interpretation: "warfarin (COUMADIN) Tablet 2 milligram Oral daily for 1 Times."
"Oral daily for 1 Times?"
Below and not indented as is the selection, where the clinician is liable not to look very carefully, is the helpful interpretation: "warfarin (COUMADIN) Tablet 2 milligram Oral daily for 1 Times."
"Oral daily for 1 Times?"
This drug needs to be given daily, generally for a very long term. Its effect on blood clotting varies for numerous reasons in an individual over time, and needs to be checked frequently via a blood test (International Normalized Ratio or INR) to ensure the level of effect is neither too little (which could result in clots) or too much (which could result in serious or fatal bleeding).
In this case, the clinician wanted Coumadin to be administered "daily", as in "each and every day", but this was the default - daily, but only once. "Oral daily for 1 Times."
Brilliant!
Brilliant!
Daily Coumadin (i.e., daily EVERY DAY), the clinician related, could be ordered only with "painstaking difficulty."
"X mg Oral daily once" is an unimaginably absurd and bizarre dosing selection to have on a CPOE system for such a critical drug - or any drug. "Daily - once?"
It should not, and does not, take a rocket scientist to realize this selection could quite easily lull the busy clinician into believing they have selected a dose to be continued every day - i.e., "once daily" - as per the standard usage of this drug.
To order this drug for (true) daily administration, a user must find a "repeat" icon and click the number of days the drug is to be administered. The "repeat" icon is not readily apparent amidst screen clutter.
For other drugs, the order choices are "## mg oral daily" or similar.
This semantic and human-computer interaction ineptitude is truly a disaster waiting to happen, especially with the medical/nursing/trainee staff turnaround that goes on in hospitals, and with the reality that clinicians are working at various hospitals with different CPOE/EHR systems.
Is this some sort scheme to prevent endless-administration Coumadin errors when the drug is actually deliberately discontinued, I ask? If so, it's ill-conceived and dangerous at best.
By way of further information, this drug is a common anticoagulant whose use is often protective of injurious or fatal blood clots that can cause strokes or death in people with common conditions such as atrial fibrillation or prosthetic heart valves:
Warfarin is used to decrease the tendency for thrombosis or as secondary prophylaxis (prevention of further episodes) in those individuals that have already formed a blood clot (thrombus). Warfarin treatment can help prevent formation of future blood clots and help reduce the risk of embolism (migration of a thrombus to a spot where it blocks blood supply to a vital organ).
The type of anticoagulation (clot formation inhibition) for which warfarin is best suited, is that in areas of slowly-running blood, such as in veins and the pooled blood behind artificial and natural valves, and pooled in dysfunctional cardiac atria. Thus, common clinical indications for warfarin use are atrial fibrillation, the presence of artificial heart valves, deep venous thrombosis, and pulmonary embolism (where the embolized clots first form in veins).
This is an example of the kinds of mission hostility (other equally bizarre examples presented here) that results when amateurs attempt to play doctor.
I add that this type of "errorgenicity" is inexcusable. If patients suffer harm from this type of "feature", the net of liability needs to go further than just the clinician who was caught in a web of cybernetic clinical toxicity.
-- SS
5/1/2012 Addendum:
More EHR madness and another physician, a cardiologist and electrophysiologist, who also believes these should be considered medical devices.
From DrWes blog (excerpts, and emphases mine; see entire post at link below):
The Electronic Medical Record Should be Viewed as a Medical Device
Apr. 30, 2012
This week I received a medical record from a large academic medical center somewhere in the United States (the details were are unimportant) that has one of these new pioneering EMR systems manufactured by $13 billion-dollar company, Cerner Corporation ... what I saw was one of the better examples of how EMRs are contributing to misinformation and confusion when health care is delivered.
I received a copy of an internal medicine consult that was performed on a patient at this outside hospital. I have extracted the "medications" portion of the internist's note exactly as it was displayed in the note below ... Needless to say, I was terrified at what the system had listed as the patient's medications:
In this example, we see multitudes of medications listed more than once. We see drugs of similar classes (antihistamines, beta blockers) on the same list. We see warfarin, one of our most dangerous drugs dispensed, without a dose included. We see what seems to be outpatient meds listed with inpatient meds, I'm not sure. Honestly, we really have no idea what medications are actually being taken from this list. And yet this list of medications is listed by the EMR as the patient's "Active Medications."Med list (page 1). Click to enlarge; see original post for part 2.
... What the heck have we created?

Certainly, any capable physician who cares for patients would describe this medication list as worthless.
This "med list" is similar to the list I showed at part 4 of my multi-part series on the mission hostile user experience of most commercial EHR's, from yet another system, redrawn by me in redacting the vendor ID. These lists reflect a mercantile computing person's view of a med list as an inventory of pills:

Another "what the heck have we created?" EHR med list, on screen. Click to enlarge.
Dr. Wes also asks:
... So how will we measure problems with EMRs? It seems industry representatives would rather not address these concerns. We should ask ourselves, is anyone thinking about this?
-- SS



